Angels in the Medical Field
A look into the world of hospital chaplains and the role of religion in medicine
-

- Photo by Chris Chapman
Reverend Lindsay Bona

-

- Photo by Chris Chapman
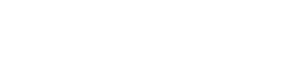
Religious practices and their accompanying hospital codes. Every patient is asked their religious preference at intake.
-

- Photo by Chris Chapman
The chapel in Mott Children's Hospital
-

- Photo by Chris Chapman
The chapel in Mott Children's Hospital was recently renovated. Cool colors and lighting were chosen to imbue serenity. Minimalist features and no religious symbols or iconography allow this space to be a place of reflection and prayer for people of all religious backgrounds.

-

- Photo by Chris Chapman
Each chapel contains a book in which thoughts and prayers can be written. When the book is full, it is burned -- in Reverend Bona's words, "sending the prayers to God."
-

- Photo by Chris Chapman
The main hospital chapel is a non-denominational space that allows for services in multiple traditions.
-

- Photo by Chris Chapman
The main hospital chapel. Although the hospital religion program encourages diversity and inclusion, not everyone agrees with this approach. The chapel was at one point victim to a theft, in which all books, icons, rugs, and kneelers were stolen. The only items left were Protestant bibles.

“How are you feeling today Katherine?” beamed Reverend Lindsay Bona as she stood at the corner of the patient’s bed, kind eyes glistening from behind dark plastic glasses. Her mundane, dark shirt and tan khakis belied her ecclesiastic position, and had it not been for her ID card dangling about her left chest, one might have mistaken her for a member of the family.
“Fine,” replied the young girl in a moth-eaten voice, eyes glued to the TV overhead. Through her translucent scalp ran sinuous veins like azure rivulets, plainly visible even in the homely light of 7th Mott.
“Ya, she’s doin’ just fine,” chimed in the child’s mother, perched on the corner of the bed opposite the reverend, a smile wearily stretching across her face, more for her daughter than herself.
“And how are you holding up?” inquired Rev. Bona of the mother, astutely noting the latter’s hunched shoulders and listless eyes.
“Oh you know… don’t wanna be here. Hopefully we’ll be out soon though.”
The conversation continued for a few minutes, Reverend Bona warmly laying out pleasantries and smiles like a mother unfurling a blanket over a child. At the close, she asked if the mother would like to pray. After receiving an affirmative, all three deferentially bowed their heads, and Reverend Bona began her invocation: “Dear God, we ask that you bless…” The TV flickered overhead as hordes of people continued to stream by the open door, oblivious to the serene scene within.
***
All of us undoubtedly have some notion that there is a priest or reverend employed at most hospitals. The typical image that comes to mind is of a wizened old man, white clerical collar bright against an ink-black cassock. Lindsay Bona, a casually dressed 30-year-old blonde, does not fit the stereotypical bill.
Raised in upstate New York in a religious household, Lindsay Bona always knew she wanted to “work for God.” By the age of 10, the precocious future chaplain was already teaching Sunday school classes at her local church. Desire to spread the word of god led her to attend Hope College in Western Michigan, with the intent of becoming an agricultural minister to Africa. Unfortunately, though strong faith she had, a mastery of biology she had not – a “C” in the class rudely terminated her plans. Abandoning her studies in the sciences for religion, hospital chaplaincy struck her as a happy medium between her two passions.
So now, instead of Africa’s green hills, jungles, and sweltering cities, her days are spent trekking through the University of Michigan Hospital. Mornings find her in the Cardiac Intensive Care Unit (CICU) working with adults. In the afternoon, she sees kids over at Mott Children’s Hospital.
Location and age are not the only things that vary from morning to afternoon – in Rev. Bona’s experience, the very concept of religion has a different character in adults and children. The former, while perhaps more articulate, sometimes have “toxic faiths” which can be detrimental to their physical health. The idea that illness ushers from God’s hand as punishment for one’s sins leads some patients to give up on themselves, to view their ill-health as a plight they must bear and not try and overcome.
Parents’ faiths can also be obstacles in their children’s convalescence. When shadowing Reverend Bona one afternoon, we entered the room of a particularly buoyant child, less than a year old, raucously bouncing around in some obviously enthralling plastic stroller/play-pen hybrid. He squealed and squirmed under the watchful gaze of mom and grandma, the former seated on a chair next to the door, the latter half-standing, half-kneeling on the side of the bed.
“Hello, my name is Lindsay Bona, one of the chaplains here,” introducing herself as we entered.
After a brief moment of incredulous silence, the mother returned a cool “hello.” Not deterred, Rev. Bona inquired as to their religious affiliation. “We’re Catholic,” volleyed the grandmother.
“Well, if you like I can inform the priest that you are here – would you like me to do that?”
“Oh yes, that would be nice.”
Rev. Bona stooped down to jabber with the pleasantly oblivious child for a few moments. Upon getting up and turning to leave, the grandmother not so much asked as grunted “So you’re the chaplain, huh?”
“One of them, yes,” replied Rev. Bona in a warm voice, obviously cultivated from innumerably similar past experiences.
“How old are you?”
“30.”
“Huh… pretty young.”
“Yes, I suppose,” she replied with the same amiability as when she first entered the room, and with one last broad smile at the child parted by saying, “Well I’ll inform the priest that you’re here – have a nice day.”
While not all parents are as ornery, in Rev. Bona’s experience, children are reliably much more open and inclusive when it comes to faith. To use her words, the faith of youth is “purer.” Free from dogma and years of inculcation on how one ‘should’ conceptualize god, some of Rev. Bona’s most powerful experiences have come from her smallest patients. She told us of a preschool-age girl, who after being prompted by Rev. Bona to draw what she thought God looked like, sketched a simple beam of yellow light. Similarly stirring was the story of a young boy, who completely devoid of any hubris or tincture of bragging, told her that Jesus had come, sat on his bed, and talked with him.
Though adults are perhaps more circumscribed in their conceptions of God, the sheer number of widely divergent religious identities seen at the hospital denies any comparative simplicity. As all the chaplains are allowed and encouraged to care for any who seek them out regardless of religious affiliation, they must all be familiar with the idiosyncrasies of various faiths. To help her discern what they may potentially desire of her, all patients are asked on their intake forms to identify their religious affiliation.
Sometimes the information is helpful. In the case of the Catholic family mentioned above, Rev. Bona was prepared for a polite rebuttal, as in her experience Catholics prefer being seen by Catholic priests. Similarly, Orthodox Jews are typically adamant about dealing solely with Rabbis.
In many cases, however, religious affiliation does not equal religious exclusivism. Hindus are actually some of her favorite people to see. “They’re great,” she said, “they usually ask me to pray with them using Jesus’ name. They want me to pray to my god because to them, it’s just another god.” Even patients self-identifying with a group seemingly hostile to a reverend, such as Atheists, often times like to talk with the chaplains. While they typically decline offers to be prayed for, they nevertheless enjoy the company and compassion displayed by the hospital-roving ministers. And for every Catholic who scoffs at anyone but an ordained priest, there are those that openly welcome any man (or woman) of the cloth.
Because patients’ wants do not always categorically correlate with their religious identification, Rev. Bona does not rely solely on this information to give her a leg-up on what to expect during the day. Instead, before going up to the wards Rev. Bona breaks down her list of patients into two categories: blue highlighter indicates those she has seen before; yellow for new patients. More often than not, these fluorescent streaks are more informative than whatever religious affiliation is printed next to the patients’ names.
***
Though it may not always be of much worth, that there even is a portion of the intake form dedicated to religion is evidence of a great sea change in the medical field regarding religion. To state that religion and science have been at odds for a few centuries is news to no one. What is perhaps surprising is that the two have much deeper historical commonalities than incongruences, and were in fact largely indistinguishable for millennia. The language of the ancient Greeks, from whom Western medicine traces its lineage, bears witness to this non-duality: “the words for saviour (soter) and for health (saos) both derive from the same root (sozo) meaning to make whole.”1 That the foundation of our medicine rests upon the bedrock of this belief is evinced by our words heal, hale, holy and whole, all stemming from the root hal, meaning ‘entire’ or ‘complete’.2
While for many years physicians have not readily recognized this, to Rev. Bona and the countless patients seeking her and her fellow chaplains out, the full meaning of ‘healing’ is plain. Recently, however there has been a strong push to critically analyze the role religion plays in health care. One of the first such forays was a paper entitled “Positive Therapeutic Effects of Intercessory Prayer in a Coronary Care Unit Population.” Published in 1988, the study reported, as its title suggests, that intercessory prayer – the act of soliciting divine intervention for the benefit of another – does have a positive, measurable effect on the healing process (which the author made sure to thank God for in the closing acknowledgments).
Since then the efficacy of intercessory prayer has been hotly debated within the medical community. Papers corroborating the seminal 1988 paper have ping-ponged back and forth with those repudiating it, though in recent years it seems the scientific validity of intercessory prayer has largely been debunked. A 2009 review found that “although some of the results of individual studies suggest a positive effect… the majority do not.”3 In fact, one study even came to the perplexing conclusion that “receiving intercessory prayer was associated with a higher incidence of complications.”4
But to Rev Bona, her fellow chaplains, and most importantly to those who seek them out, such statistical proofs are as esoteric and devoid of relevancy as science holds religion to be. Indeed, a USA Today/Gallup Poll conducted in May of this year showed that 83% of those surveyed believe “there is a God who answers prayers,”5 revealing just how substantive prayer is in the American psyche. For most Americans, the objective efficacy of the experience matters little, for what cannot be doubted in their minds is its subjective import.
What is also clear is that physicians are ill equipped to provide this aspect of patient-care. For one, the role religion plays in the lives of physicians and the American populace at large is widely divergent. A recent study by Dr. Farr Curlin of the University of Chicago found that physicians were less likely to “look to God for strength, support, and guidance,” and also more likely to “try and make sense of [a] situation and decide what to do without relying on God.”6 Further, physicians, even when sympathetic to patients’ desires for spiritual attention, do not feel comfortable providing it. Another study by Dr. Curlin found that while only 17% of physicians said it was “never appropriate for a physician to pray with a patient,” 47% nonetheless “never pray with patients,” even when the patient broaches the subject.7
The gravity of such data has not been lost on medical educators. The AAMC has made it a point to bring religion into the medical curriculum under the umbrella of ‘cultural competence’. A cursory search through the back-issues of Academic Medicine reveals frequent calls for increased exposure to religion during medical students’ pre-clinical years. For us at Michigan, this occurs for approximately ten minutes between the hours of 9 and 11 am on Thursday mornings, and consists largely of discussing how to deal with patients whose religious beliefs affect the normal course of treatment. Unless Step 1 of the USMLE is re-vamped to include a section on cultural competency, it is doubtful whether any time spent on the issue will have an appreciable impact on how ‘competent’ medical students actually are in caring for the spiritual needs of their patients.
***
The chaplain’s indispensability, then, seems secure for the near future. In fact, as the science of medicine continues to crowd out the more ephemeral ‘art of medicine’, the role of the hospital chaplain continues to increase. At Brigham and Women’s and Massachusetts General, both standard-bearers of ‘evidence-based medicine’, requests for chaplains over the past few years have jumped 23% and 30%, respectively.8 Because of this high demand, around the country chaplains like Rev. Bona are now required to have pagers and take call.
Even as their clinical responsibilities increase, they are also called upon to perform a variety of other duties in the hospital. Part of working on 7th Mott for Rev. Bona entails attending Psychosocial Rounds, a collaboration between psychologists, physicians, social workers, nurses, and chaplains. Another one of the chaplains serves on the hospital’s ethics committee. Rev. Bona also told us that there is a push from within the chaplaincy to start performing quantitative research.
But whatever new realms chaplains venture into, patient care must surely remain at the core of their duties. A devout Christian all her life, Rev. Bona told us she felt “God more present in the hospital than in the church;” odd, perhaps, considering the diverse amalgamation of religions represented in the hospital. The truth of Rev. Bona’s statement lies in the fact that, while fractured by labels, the hospital’s population – from patients to their families to staff – are united in their confrontation with suffering. Here, in this shared experience, this universal human emotion, cracks the mundane veneer of life, a fissure through which “listening for God,” as Rev. Bona put it, is possible.
- Sevensky, RL. “The religious foundations of health care: a conceptual approach.” Journal of medical ethics, 1983, 9, 165-9 [↩]
- Ibid. [↩]
- Roberts L., et al. “Intercessory prayer for the alleviation of ill health.”Cochrane Database Syst Rev., 2009 April 15; (2):CD000368 [↩]
- Benson, H., et al. “ Study of the Therapeutic Effects of Intercessory Prayer (STEP) in cardiac bypass patients: a multicenter randomized trial of uncertainty and certainty of receiving intercessory prayer.” Am Heart J. 2006 Apr;151(4):934-42. [↩]
- http://www.pollingreport.com/religion.htm [↩]
- Curlin, Farr A., et al. “Religious Characteristics of US Physicians: A national survey.” J Gen Intern Med. 2005 July; 20(7): 629-634 [↩]
- Curlin, Farr A., et al. “The association of physicians’ religious characteristics with their attitudes and self-reported behaviors regarding religion and spirituality in the clinical encounter” et al., Medical Care, May 2006, Vol 44, Issue 5, pp 446-453 [↩]
- http://www.boston.com/news/health/articles/2009/08/31/more_patients_seeking_spiritual_guidance_from_chaplains/?page=full [↩]
No comments yet.
RSS feed for comments on this post
TrackBack URI