The Heart of the Mayan World
A caravan of boxes
-

- Photo by Sam Terman
Lake Atitlan early in the morning.

-

- Photo by Sam Terman
A view up the active volcano Mt. Pacaya.
The evening we landed, I placed a phone call. At the end of the conversation, a sleepy voice ebbed, “Glad you’re there. But honey, just don’t go into any volcanoes.” Mothers are required to worry, but clearly we were far from home. Mothers are always right: I have a feeling that the smoldering lava beneath my feet had stolen at least a hair of traction from my tennis shoes.

-

- Photo by Sam Terman
Our Spring Break 2010 service-learning trip to Guatemala consisted of seven eager first year University of Michigan Medical School students (Sam Terman, Nirmish Singla, Liz Chenoweth, Jackie Madison, Chris Eisert, Yorgos Stranga, Yushen Qian), one internal medicine physician (Dr. Joyeeta Dastidar), and one medical translator (Paz Angelica Snyder).

-

- Photo by Sam Terman
Dr. Garcia explaining medications to a patient.

-

- Photo by Sam Terman
An examination room in a Guatemalan clinic.

-

- Photo by Sam Terman
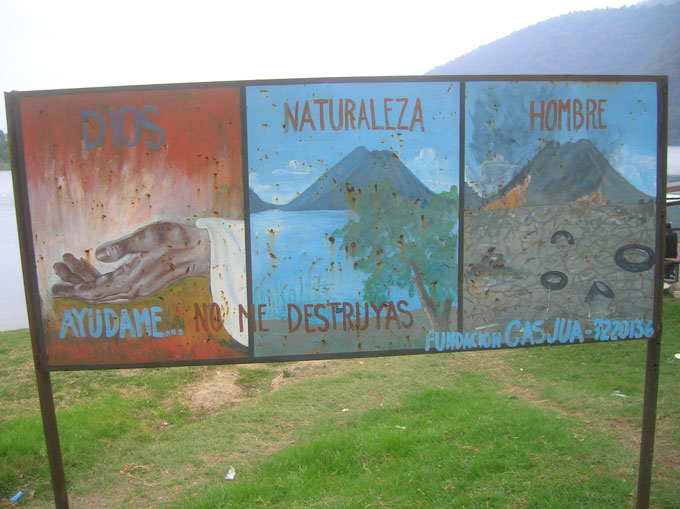
The life cycle explained in images.

-

- Photo by Sam Terman
A revolutionary reminder.

-

- Photo by Sam Terman
The Mayan-Christian god, Maximon.

-

- Photo by Sam Terman
Paintings surrounding Lake Atitlan.
-

- Photo by Sam Terman
Sunset over the Pacific Ocean.

-

- Photo by Sam Terman
We departed Antigua for the airport at a morning hour when even the roosters were sure to be fast asleep. But another week’s curriculum of Clinical Foundations of Medicine and conquering the musculoskeletal physical exam drew us back to Ann Arbor. I shut my eyes as we jetted back into the sky and thought about how next time I’ll be sure to bring marshmallows for toasting at the top of Volcan Pacaya.

In February 2010, we entered as a marching caravan of boxes. Heaving taped cardboard stuffed with donations of acetaminophen and Ziploc baggies, oral rehydration and omeprazole had journeyed thousands of miles now plunging into the Heart of the Mayan World. The customs worker systematically popped open each container, thanked us for the work we were doing for his country, and shuffled us out of the Guatemala City airport’s dimly lit corridors and into an unfamiliar land.
Our destination was the San Lucas Mission, a non-profit NGO situated on the picturesque Lake Atitlan in the Guatemalan Highlands. Originally founded by the Franciscan order in the late 16th century, the Mission was reinvigorated in 1958 by launching a diocesan partnership spanning from Minnesota to Guatemala. Since then, the Mission transformed what was once a village of thatched huts without electricity or plumbing on the verge of civil war, where non-existent access to education (literacy rate 2.5%) ensured that the local Mayan population could find work only coffee plantations and where healthcare was an ancient indigenous art, into a town with stone homes, schools (literacy rate now 85%), and doctors. Charged with its purpose to “respond, as Jesus did, to the needs of the people,” the Mission offers programs in food security, potable water via hydroelectric pumps from Lake Atitlan, occupational apprenticeship programs, and free outpatient clinic services.
While the Mission’s progress was inspiring, daunting economic, sociocultural, and healthcare challenges remain abundant. In a country where half of the population lives on less than $2 per day, poverty is an activist’s worst enemy. Though the Mission is building a Women’s Center, our tour guide informed us that women are triply discriminated against for being female, poor, and indigenous. Cultural and historical tension lingers from 19th century policies which established a 2% economic elite owning 80% of the land. The Mission has now charged itself with returning land to its ‘rightful’ Mayan owners. The maternal mortality rate is virtually 20 times that of the United States, and physician supply is just over a third of what the World Health Organization considers adequate.
I had done my homework. But as the airplane thudded safely to the ground in Guatemala City as I peered out of the airplane’s push-up window at nighttime darkness studded with lights whizzing by, I still felt like a fish dropped into a vast unfamiliar ocean. “Whelcome to Whatemala” said the overhead. I wondered what I could possibly do to fulfill the ‘service’ portion of our service-learning trip, with incomplete medical training and six days to save the world. My homework reading scared me. I wondered if I would fall prey to ‘Duffel Bag Medicine.’ The Duffel-Bagger is a self-aggrandizing foreigner wearing a cowboy hat and ripped jeans and smoking a cigarette dispensing medications without competence or accountability. He or she ultimately irresponsibly hurts the vulnerable target community. I possessed shoddy communication skills despite helpful Medical Spanish classes, was nearly oblivious to the complex local culture, and was hoping to pat myself on the back at the end of the week for using my vacation to do good. But I refused to accept the ‘Duffel Bag’ mindset. I may not be here to save the world, but I was ready for an experience testing the limits of Western medicine in a country whose challenges run far deeper than health care.
For three days, we zipped on the back of a pickup truck each morning along with med students from USC and WVU to staff rural clinics run by the Mission – Quixaya, El Naranjo (literally “the Orange”), and Pampojila. Auscultating hearts and lungs, taking patient histories, and dispensing medications and vitamins quickly became routine. Fussy babies had earaches and pneumonia, and mothers dressed in brightly mottled red, purple, and blue dresses listened intently as we explained how to take her free of charge albendazole and the importance of sanitation, hydration, and nutrition. Makeshift exam rooms were composed of shoved-together benches, with the occasional examination bed, and La Farmacia consisted of a card table planted next to a plastic tub swimming with medications. Patient records were scribbled on index cards assembled in haphazard alphabetical order. At a house call for a family elder, children looked on intently from behind the cracks as Dr Garcia, eyes focused in a downward stare, palpated their stoic grandmother’s apple-sized lymph nodes. It was cancer, and the only available and feasible treatment was bed rest and comfort. Serving the people’s most basic needs far from the closest MRI machine, where high-end treatments are more often than not economically and physically out of reach and basics like stool samples and blood cultures are not readily available, we were far from the privileged ivory tower of academic medicine.
My Guatemala is also a place of breathtaking Pacific sunsets and lakeside motorboat rides, where women hike mountainous dirt trails even more seamlessly balancing baskets atop their heads with every generation. It is where coca cola comes in glass bottles containing a smoother and sweeter sugar, zealous roosters’ cries wake you up several times every morning, and you’re never sure looking up at active volcanoes whether you are seeing mountains kissing wispy clouds or ominous smoke rising. Tourists and tuc tucs [small motor cars] buzz past bustling marketplaces boasting beans and malodorous “fresh” seafood, bicycle bells and chicken brains where you can walk all morning only to end up exactly where you began. There are stretches of road segregating drug dealers from their buyers and stretches of road studded with cobblestones and Baroque churches radiantly illuminated at night. Guacamole, fried plantains, and cinnamon ice cream make you never want to leave.
If the Lion King teaches us anything, it is that there is more to see than can ever be seen in a lifetime, let alone a week. We observed a minutiae of the country’s deeply ingrained cultural and religious past, awe-inspiring sights and adventurous attractions, and socioeconomic and health disparities. But I felt that I had accomplished much in a short period of time – if not because of my contributing medical expertise, in terms of deepening my understanding of health care delivery in a developing country and enhancing my clinical skills in a primary health care setting. I didn’t feel like a Duffel Bagger or a do-gooder. I felt like a student of medicine and international health just starting to blink and stepping into the sun. My first international health experience and opportunity to practice delivering care beyond the confines of the University of Michigan’s Learning Resource Center, this trip’s greatest service was through learning, a formative educational experience beyond what textbooks, articles, and statistics could possibly offer.
No comments yet.
RSS feed for comments on this post
TrackBack URI